Now Reading: Is 3D Printing the End of Traditional O&P?
-
01
Is 3D Printing the End of Traditional O&P?

Is 3D Printing the End of Traditional O&P?
I’ll never forget the look on two different patients’ faces, years apart, as they experienced two different realities of my profession.
First, there was Hanif, a retired carpenter who lost his leg below the knee to diabetes. I remember the grimace on his face as we applied the cold, wet plaster strips to form a cast of his residual limb. It was messy, uncomfortable, and to him, it must have felt archaic. We were building the foundation for his new life with a technique centuries old.
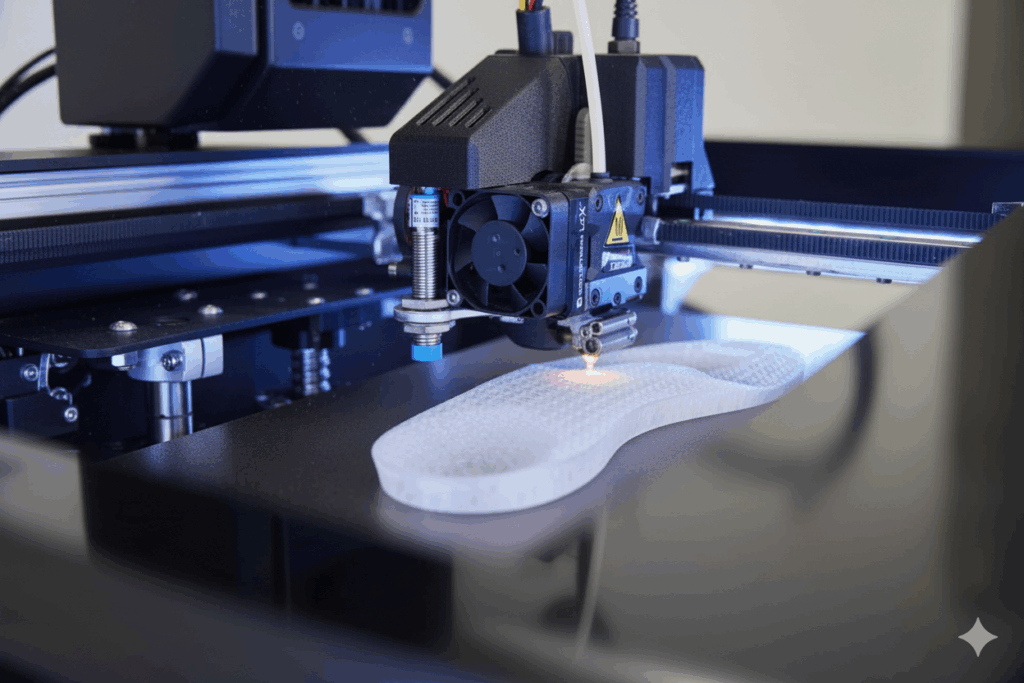
Then, there was Sarah, a young artist who needed an ankle-foot orthosis (AFO). Instead of plaster, she saw the soft red light of a 3D scanner gliding over her leg, capturing every contour in a silent, digital dance. On the screen, a perfect 3D model of her anatomy rotated. Later, she watched, mesmerized, as her custom AFO—a intricate, lattice-work design that looked more like a piece of modern art than a medical device—was born layer by layer from a 3D printer.
These two moments exist in a single career, and they frame the central question facing my field today: Is 3D printing the end of traditional Orthotics and Prosthetics (O&P), or is it simply the next, inevitable chapter in our story?
To understand the future, you must first respect the past. Traditional O&P is not just a manufacturing process; it is a clinical art built on a deep, tactile dialogue with the patient.
When I hand-sculpt a plaster mold or modify a thermoplastic socket with a heat gun, I’m not just shaping a material. I’m translating what I see, feel, and hear. I’m observing how a patient’s muscles contract during the gait cycle, feeling for pressure points through the socket, and listening to their feedback: “It’s tight here when I sit down,” or “It pinches there when I pivot.” This is the “dynamic fit”—a living, breathing process that a static digital scan cannot, on its own, comprehend.
The materials we’ve relied on for decades—carbon fiber, acrylic resins, thermoplastics—are incredibly versatile and durable. They can be modified in minutes. A quick grind here, a spot of heat there, and we can make an adjustment that would require a full re-print in the digital world. This instant, intuitive repairability is a form of “real-time editing” that remains a formidable strength of the traditional craft. It’s the embodiment of clinical experience made physical.
Now, enter the disruptor. 3D printing, or additive manufacturing, isn’t just a new tool; it’s a new philosophy. Its advantages are profound and, in some areas, revolutionary.
- The Perfect Digital Mold: The 3D scanner is a game-changer. It captures millions of data points in seconds, creating an flawless digital replica of the anatomy without the discomfort of plaster. This file is permanent, can be perfectly replicated, and emailed across the globe.
- The Weightless Advantage: This is where the magic truly happens. Using a process called topology optimization (think of it as software that designs structures with the intelligent efficiency of a honeycomb or a bird bone), we can create devices that are incredibly strong yet astonishingly light. We put material only where it’s needed for strength, leaving elegant, hollow lattices everywhere else. The result for patients like Sarah is an AFO that is less of a burden and more of a natural extension.
- The Customization Revolution: This goes far beyond simple fit. This isn’t frivolous; it’s a powerful psychological tool that transforms a medical device into a personal statement, dramatically improving acceptance and adherence, especially in pediatric care.
- The Digital Thread: The entire workflow becomes streamlined and data-driven. A patient’s file can be stored forever, modified with a few clicks to accommodate weight loss or growth, and printed on-demand. This holds the promise of revolutionizing care for underserved communities through telemedicine, where a local clinic with a printer could produce a device designed remotely by a specialist.
Here comes the question that Where the Printer Stops ? For all its brilliance, the 3D printer is not a magic box. As a clinician, I must be brutally honest about its current limits.
- The Material Gap: While improving rapidly, the layer-by-layer nature of 3D printing can sometimes result in parts that aren’t as durable or fatigue-resistant as the continuous fibers of a carbon composite or the strength of titanium. For a high-impact prosthetic leg for an active adult, the material science isn’t always there yet.
- The “Static Scan” Problem: This is the critical counterpoint to the digital mold. A scan is a snapshot of a limb at rest. It doesn’t know how the soft tissue will bulge and stretch under the load of a body walking. This is where the clinician’s expertise is irreplaceable. We must digitally “rectify” the model—a process of virtually pushing and pulling the digital tissue based on our understanding of biomechanics. Without this clinical interpretation, the most perfect print will be uncomfortable.
- The Speed Illusion: People think hitting “print” is instant. It’s not. Designing a complex, lattice-structured device can take hours. The print itself can run for 12, 18, even 24 hours. For a single, complex device, this is revolutionary. For a busy clinic that needs to turn around five standard AFOs in a day, traditional methods are often still faster.
- The Cost of Entry: The investment isn’t just in the printer. It’s in the scanner, the sophisticated software, and, most expensively, the time and training required to upskill a whole team of clinicians.
So, where does this leave us? With a synthesis that is more powerful than either approach alone. The future O&P professional is not a craftsman , but a “Digital creator.”
Our role is evolving. We use our clinical expertise to diagnose the patient’s unique functional and psychological needs. We use the scanner to capture perfect anatomical data. We then step into the digital realm, using our hard-won knowledge of biomechanics to sculpt, optimize, and rectify the virtual design. We command the printer to fabricate this precise blueprint. Finally, we return to our roots, using our traditional skills to perform the final, dynamic fitting, to align the device perfectly to the patient’s gait, and to provide the education and empathy that no machine ever can.
The technology is a powerful tool that augments clinical judgment; it does not replace it. Let me be clear: the most dangerous person in O&P is someone with a 3D printer and no clinical license.
Let’s return to Hanif and Sarah. The ideal future isn’t one where Hanif’s experience is obsolete. It’s one where his digital scan is captured comfortably, his socket is printed with a perfect, personalized fit, and then brought to life by a clinician’s experienced hands for the final, dynamic alignment. It’s the marriage of digital precision and human intuition.
So, is 3D printing the end of traditional O&P? No. It is the end of traditional O&P as a purely analog craft. It is transforming our noble profession into a hybrid digital-physical discipline.
The ultimate goal remains unchanged: to restore mobility, function, and, with it, dignity. 3D printing is not the end of our story. It is a new, profoundly powerful tool in our arsenal, allowing us to serve our patients with greater precision, deeper personalization, and more passion than ever before. And that is a future worth building, layer by layer.